

The Origins of Echocardiography
One doctor's perseverance from humble beginnings revolutionizes the way we diagnose cardiac disease.

The following includes excerpts from The POCUS Manifesto: Expanding the limits of our physical exam with point-of-care ultrasound. I was lucky enough to interview the father of echocardiography, Dr. Harvey Feigenbaum himself, via Zoom.
—
Situated in the southwest tip of Sweden sits the city of Lund, where two cardiac surgeons - Drs. Helge Wulff and Phillip Sandblom - were operating on patients with severe mitral stenosis (a pathologic narrowing of the valve) in the 1940s. Once the chest was opened and the mitral valve revealed, the surgeons would dilate the narrowed valve with their fingers, causing many patients to improve. However, some patients also had a component of mitral regurgitation, a leaking of the valve that worsened with this finger dilation. This created an opportunity for Dr. Inge Edler, a physician from Malmö who moved to Lund to become the director of this cardiovascular lab at the University Hospital, responsible for pre-operative cardiac evaluations. He was tasked with determining which patients had pure mitral stenosis and would benefit from surgery, yet there was no good method for identifying these patients at the time.

Edler was an amateur magician, an avid bicycle acrobatist till the age of 75, and an overall curious man with varied interests. As scientists around the world were looking to repurpose wartime technologies for other uses after World War II, Edler hypothesized that one of those technologies, sound navigation and ranging or SONAR, could help with his clinical dilemma. He consulted with his clinic nurse who was married to a physicist, and her husband, in turn, thought of a friend who may be able to help: a man named Hellmuth Hertz.
Hertz came from a distinguished pedigree of physicists, with his father winning the Nobel Prize in Physics. Not to mention his uncle, Heinrich Hertz, the same Heinrich Hertz that lent his name to the unit of frequency. Dr. Edler presented his idea of using sonar-based ultrasound to study the heart to Hertz who was intrigued, and thought ultrasound may work (Interestingly enough, Hertz had previously consulted with Dr. Edler as a patient seeking advice for his headaches). In 1953, they went to a shipyard nearby that had an ultrasound machine. Hertz placed the probe on his chest and a moving signal appeared. The first cardiac ultrasound, he wondered? By pure luck, this machine happened to have a transducer with the correct wavelength to see the heart. If it were lower or higher, they may not have detected anything.
To understand exactly what he was seeing on this new ultrasound device, Edler would conduct clever yet morbid sonographic exams on patients near death. He marked the direction of the ultrasound beam on the patient’s chest, and when they passed away, he passed an ice pick through the chest wall in the direction taken by the ultrasound beam. Then on autopsy, he traced where in the heart the ice pick had pierced and compared that distance to the distance of the ultrasound signal on the screen. He figured out that the tip of the ice pick had entered through the mitral valve, which was causing the signal in question, and was eventually able to identify the signal a stenotic mitral valve made compared to a regurgitant one.

Just as with other medical pioneers who came before them, there was a cold reception for Edler and Hertz’s discovery. They presented their methods to Dr. Andre F. Cournand, a physician who received the Nobel prize for his contributions to cardiac catheterization, who was not impressed. They also showed it to President Dwight D. Eisenhower’s cardiologist Paul Dudley White who politely dismissed it as unimportant. Likewise, they could not get funding from the Swedish Board of Technical Development, because they believed it lacked medical or commercial interest.
These rejections proved insurmountable, and Edler’s interest in ultrasound fizzled as his technique for identifying mitral stenosis turned out to not be very precise and was eventually discredited. Fortunately for the future of cardiac diagnostics, a very similar story was unfolding in the United States, led by a young cardiologist named Harvey Feigenbaum.
Feigenbaum’s Discovery

Like every day at work, Dr. Harvey Feigenbaum was eating lunch in his office when he came across an advertisement in a random journal on his desk. The ad was from a company named BioSonar, promoting a product that they claimed could measure heart volumes with ultrasound. It was an idea that intrigued Feigenbaum since he was struggling with the concept of measuring heart volumes during cardiac catheterizations at the time. He called the number on the advertisement and found out they’d be showing their new device at the upcoming American Heart Association meeting in 1963. Feigenbaum attended that meeting and beelined to the BioSonar booth. He eagerly asked the person working there how to use their device to measure cardiac volumes, to which the BioSonar representative responded:
“What are cardiac volumes?”
It turned out the advertisement Feigenbaum saw was quite misleading since the machine actually used ultrasound to detect the midline of the brain, not volumes of the heart. Confused as to why such a machine was at a cardiology conference, Feigenbaum placed the machine’s probe on his chest and immediately saw a moving spike. “It was obviously related to my heart ... the way it was moving, the timing of it, location of it. It had to be coming from the back wall of my heart.” Excited about his discovery, Feigenbaum wondered if it could detect a pericardial effusion.
Back at the hospital, he borrowed a similar machine from the neurology department and began examining patients with it, seeing the same, singular moving echo signal from the heart. He found a patient with a known pericardial effusion and placed it on their chest. “Just as I predicted, instead of one signal that was moving, I saw 2 signals. One was moving and the other was stationary, and the space between the two had to be the effusion.”
He called Dr. John Waldhausen, a cardiac surgeon who had an animal laboratory, and they set up a study in dogs to see if these findings could be reproduced. “We injected saline into the pericardial space and the singular signal divided into 2, one moving and one stationary. We took the fluid out and the signals or echoes came back together. We repeated this routine in 5 consecutive dogs and that was it. It happened every time.”
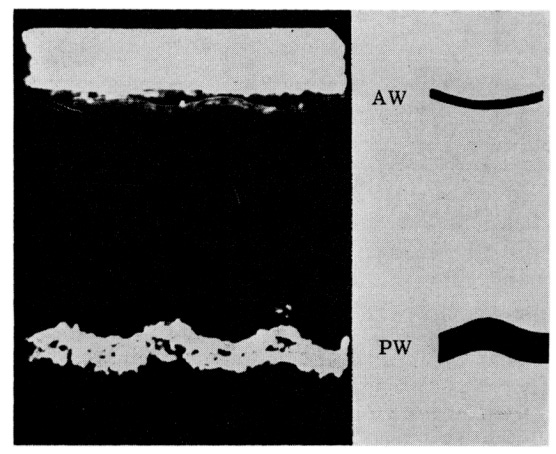
In the example below, the upper white line is a signal from the anterior wall (AW) of the heart, and the sine-wave-shaped lower line is the posterior wall (PW). In this example of a normal heart, the PW signal is just one line representing the movement of the heart and surrounding pericardium as one.
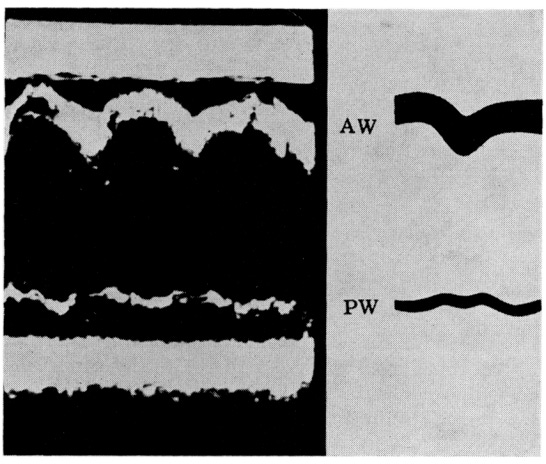
In this second example below in a patient with a large pericardial effusion, the anterior wall (AW) is one signal. However, now the posterior wall is split into two signals, separated by a pitch-black space which Feigenbaum figured out is the pericardial effusion.
They published a paper titled Ultrasound Diagnosis of Pericardial Effusion in 1965 documenting their findings, but it largely fell on deaf ears. “By the time that I came up with ultrasound, they decided it was garbage,” Feigenbaum later recalled. “The skepticism was overwhelming. I had the misfortune to follow ballistocardiography (a technique based on recording the effect of heart contraction on the body as recorded on a motion-sensitive table), which was a disaster. Skeptics said: here we go again.” Dr. W. Proctor Harvey, a famous cardiologist at Georgetown University who ran the largest and most competitive cardiology fellowship at the time “completely refused to accept echocardiography,” and was “completely wedded to the physical examination with auscultation.” Likewise, the editor of the American Heart Journal, a premier cardiology journal at the time, declined to publish on echocardiography.
Even the manufacturer of the ultrasound machine Feigenbaum was using at the time, Smith-Kline, was going to give up as well if it wasn’t for one man at the company named Tom Davis. He believed in Feigenbaum’s work and invited him to one of their marketing meetings in 1965. Feigenbaum gave a presentation arguing that “cardiac ultrasound would be a major diagnostic tool because we are “seeing the heart.” Those signals were coming from the heart! How can that not be important!?”
Dr. Edler had faced much of the same pushback and spent almost 10 years working on ultrasound but eventually gave up. “The main difference between us was that I was dead set on cardiac ultrasound and he wasn’t,” Feigenbaum explained. “Inge was a wonderful human being. We spent a lot of time together both in Europe and the United States,” but his work with echo was short-lived, and his main findings turned out to not be very useful. Despite this fact, according to Feigenbaum, his European colleagues tended to glorify Edler’s contributions and downplay his, as evidenced by the fact that the European Society of Echocardiology (now called Cardiovascular Imaging) didn't get around to making him an honorary member until 2014.
Feigenbaum’s passion and determination convinced Smith-Kline to continue making their device, enabling him to continue his work in developing the field. His work in ultrasound eventually earned him the title of “the father of echocardiography,” revolutionizing the field of cardiac diagnostics forever.
—
Dr. Larry Istrail is an internal medicine physician and author of The POCUS Manifesto: Expanding the limits of our physical exam with point-of-care ultrasound. You can buy it on Amazon here.
Brilliant .Now I understand why the M Mode is referred to as ICE PICK image.