
Sesame seed allergy: A deep dive
Sesame seed allergy: A deep dive
Who knew the main ingredient in hummus could be so dangerous?


—
Dr. Larry Istrail is an internal medicine physician and author of The POCUS Manifesto: Expanding the limits of our physical exam with point-of-care ultrasound. You can buy it on Amazon here.
—
The sesame seed is a seed native to the Middle East and Africa, usually consumed as a tahini paste in hummus, or as a delectable dessert in the form of halvah. It is in everything from crackers to hamburger buns, Asian foods to dressings, and gravies to cereals. To some, sesame seeds are the foundation of a healthy and delicious hummus spread in a summer snack, while to others they are PTSD-inducing death bombs waiting to enter your bloodstream and wreak havoc with one tiny, unassuming bite.
Sesame allergy affects anywhere was 0.1% to 0.2% of the population in the USA or Canada, to as many as 0.8% of the population in Australia. And only 20-30% of people with sesame allergy will outgrow it, as compared to relatively high rates of spontaneous resolution with milk or egg allergies. Sesame-allergic people, like anyone with food allergies, are at risk for severe and potentially life-threatening anaphylaxis reactions if they accidentally consume foods containing sesame. The reactions can range from mild swelling and hives to full-blown anaphylaxis that results in extremely low blood pressure, severe nausea and vomiting, and possibly death.
Sesame seed anaphylaxis rates vary by region, causing over 40% (6 of the 14) of the anaphylaxis cases in an Israeli cross-sectional study, while only causing 2.8% of them in Canada. These severe reactions can be absolutely devastating, taking a young previously healthy person to the brink of death in minutes. Sadly, such was the case in 2014 for example, when a 30-year-old woman with a sesame allergy traveled to Israel and died after inadvertently eating tahini. She ordered a fish seasoned with “tehina” at a Jerusalem restaurant, not knowing it was made from sesame seeds. She suffered immediate anaphylaxis, and after four days in the ICU, sadly passed away. Two years later another devastating case happened when a 15-year-old collapsed on a British Airways flight after eating a baguette from Pret-a-Manger that contained sesame seeds. Despite two doses of epinephrine administered by her dad, she sadly passed away later that day.
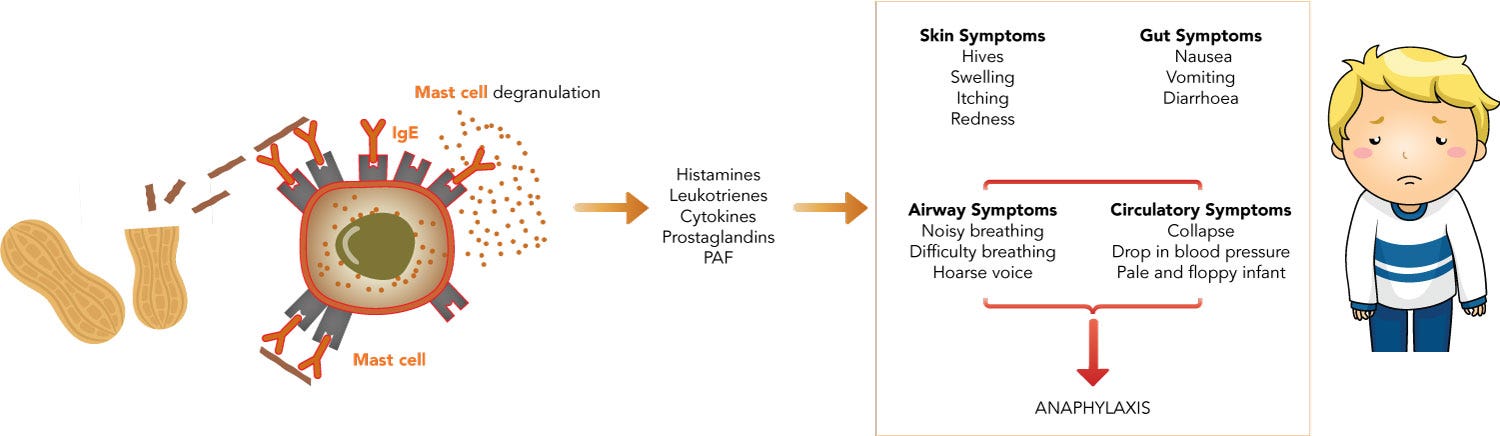
These horrendous reactions result from an inappropriately aggressive response by the immune system (called an immune hypersensitivity reaction) to the proteins inside the sesame seeds. The most common type is IgE-mediated, which manifests minutes to one hour after eating, as opposed to Non-IgE mediated, which can happen hours to days after. In IgE-mediated allergic reactions, certain white cells in your bloodstream that are primed to detect foreign particles can bind to sesame proteins and quickly produce an antibody called IgE. These antibodies then circulate in the blood and bind to IgE receptors on other immune cells called mast cells and basophils, causing them to release an overabundance of proteins and chemicals that cause vasodilation of blood vessels, mucous secretion, and smooth muscle contraction that results in low blood pressure, runny nose, or shortness of breath respectively. In 1-20% of the cases, the anaphylaxis can be biphasic, and symptoms may recur after the initial episode 1 hour to 72 hours (most within 8 hours) after the apparent resolution of the initial phase.
The immune reaction seems to be triggered by three proteins inside the sesame seed (called Ses-i-1, Ses-i-2, and Ses-i-3). The Ses-i-3 protein is about 80% similar to one in peanuts that triggers peanut allergy, which may explain why patients allergic to sesame are often also allergic to peanuts, as well as other foods like hazelnut, rye, kiwi, poppy seed, black walnut, cashew, macadamia, and pistachio. The immune system cannot detect these proteins until the seed is crushed, which is why many people with sesame allergies often report eating sesame seed bagels without developing a reaction. In addition, the oils in the sesame seed (sesamol, sesamin, and sesamolin) are responsible for contact dermatitis (allergic reaction when it contacts the skin), which can cause a problem since they are used in various creams, lotions, and other pharmaceutical products.
As of January 1st, 2023, the United States Food and Drug Administration started requiring sesame seeds to be labeled as a food allergen on all food and supplement packaging. It joins the ranks of 8 other foods that must be listed as well: milk, eggs, fish, shellfish, tree nuts, peanuts, wheat, and soybeans. While this is theoretically a win for people with sesame allergies, the incentives it has created seem to have had the opposite effect. According to the Chick-fil-a website, “[t]his industrywide matter led to a recipe change for our white bun and multigrain brioche bun to now include sesame as an ingredient.”
So… a law requiring sesame to be labeled as an allergen led them to add more sesame to their foods!?
“By adding sesame to products that didn’t previously contain it,” Jason Linde, the senior vice president of government and community affairs for FARE, a nonprofit working to increase food allergy awareness said in a Buzzfeed article, “companies may be able to skirt manufacturing processes that would ensure production facilities are clean enough to avoid cross-contact with the allergen. Or as the Center for Science in the Public Interest phrased it:

The same thing happened at Olive Garden, which explained to BuzzFeed News that “because the FDA recognized sesame as a major allergen, it has added sesame flour (‘less than 2%’ according to the company) to its famous breadsticks due to the potential for cross-contact in its bakeries.” The law of unintended consequences can be damning.
Diagnosis, Treatment & Prevention
The main way to diagnose a food allergy (apart from accidentally eating it) is through skin prick testing (SPT), where a standardized diluted sample of the allergen is placed on the skin. If a raised red wheal develops at that site, it confirms that someone has the IgE proteins specific to that allergen, yet it doesn’t confirm they will have a significant allergic reaction to it. If the wheal is 8mm or more in diameter, it is almost certain that person will have a bad reaction to the allergen (95% positive predictive value), while if it is over 3mm in diameter, it is likely but not certain (58% positive predictive value). On the other hand, if the test is negative, this essentially rules out an allergy to most allergens. Yet with sesame, another test called Skin-prick-prick (SPP) uses actual sesame seed oils or tahini instead of commercial extract and may detect some allergies that were missed with SPT.
The other standard method is a blood test that measures the concentration of sesame-specific IgE antibodies, yet the clinical utility of different levels is controversial. In one study, a level of 50 kU/L or greater had a positive predictive value of 86%. Yet the diagnostic accuracy overall was relatively low. This was also seen in another study which showed a positive serum IgE test had only 70% sensitivity and 30% specificity for diagnosing an allergy.
So, can sesame allergy be prevented?
One food allergy hypothesis suggests that lack of exposure in utero predisposes you to an allergy to that food. This is supported by a few studies including one association study which showed that the more peanut, milk, and wheat the moms ate (according to a questionnaire), the less likely the baby was to have a food allergy to those allergens.
Yet exposing the baby to sesame during pregnancy in another study of women getting fertility treatments didn’t reduce the risk, and in fact, seemed to increase the risk of sesame allergy. They used progesterone specially formulated with sesame oil, which did not increase the odds of the baby developing sesame-specific IgE in their blood. However, moms who ate sesame seeds were more likely to have a child that was sensitized (i.e. had the IgE antibody and positive skin test) to peanuts, tree nuts, or sesame seeds (odds ratio of 1.78 with a confidence interval of 1.08 - 2.92). But whether this resulted in a true increase in clinically significant food allergy is uncertain.
Apart from avoidance, the main preventive intervention is oral immunotherapy, in which the allergic patient eats an increasingly large amount of the allergen over time, starting with a very tiny amount in order to desensitize them. It is very effective for different allergens like peanuts and milk, but until recently studies with sesame seed allergies were not done.
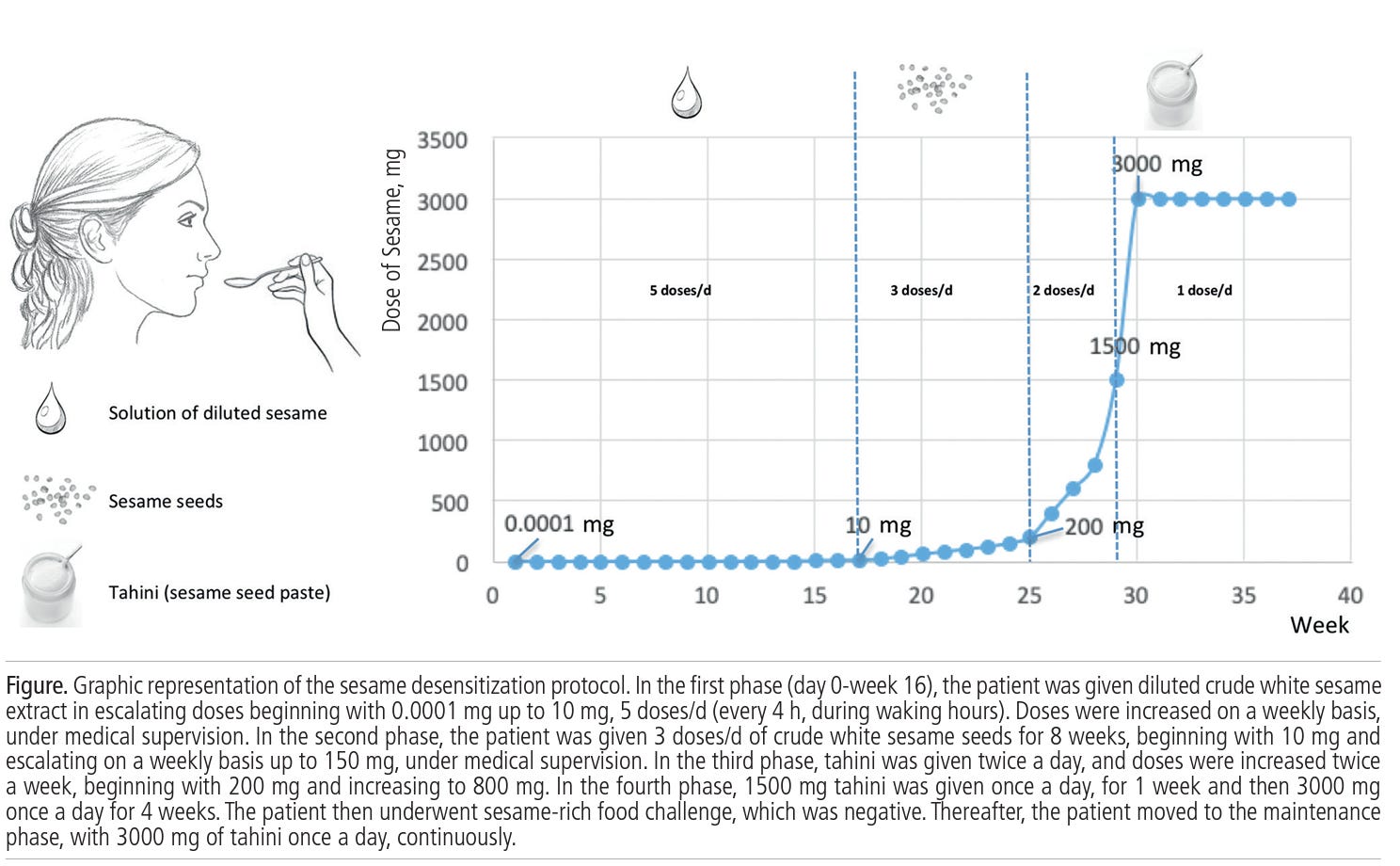
Impressive results were seen in a case report from Brazil describing successful oral desensitization in a 48-year-old woman who had 7 episodes of sesame seed anaphylaxis in a 20-year period. Starting with 0.0001 mg of sesame, she slowly increased her intake over the course of 30 weeks up to 3,000 mg. She then started a maintenance phase, eating 3 grams of tahini once per day for four weeks. After this, she underwent a sesame food challenge and had no reaction. Her skin prick test was also negative, and she was able to eat sesame-containing foods with no symptoms.
In a randomized controlled trial published in the prestigious New England Journal of Medicine, 1,303 exclusively breastfed infants were randomly assigned to introduce allergenic foods (peanut, cooked egg, cow’s milk sesame, wheat) early, at 3 months of age. This group was compared to the standard United Kingdom practice of introducing them at 6 months, finding that when comparing both groups as they were randomized (intention-to-treat analysis), food allergy to one or more of the foods developed in 7% in the standard group and 5.6% in the early group, though it was not a statistically significant difference (p=0.32).
When they broke it down by infants that followed the protocol as they were supposed to (per-protocol analysis), the rate of allergy development was 67% lower in the early introduction group (2.4% vs 7.3%, CI= 0.13 - 0.83, p=0.01). There were no cases of peanut allergy among the 310 participants in the early-introduction group, as compared with 13 cases in the control group (p=0.003). There was also a significant reduction in egg allergy, and less sesame allergy, though this wasn’t statistically significant.
There is a lot of bias that is introduced from using a per-protocol analysis that may be misleading, but these results are consistent with a large randomized trial of peanut allergy that showed an 86% reduction in peanut allergy among the infants who had about 6 grams of peanut protein per week, consumed as Bamba peanut butter puffs:

Similar results were confirmed in sesame allergy in an Israeli study published in 2019. They started with tiny doses of high-protein sesame extract and had dose escalations in a monitored setting to find the highest tolerated dose, which was then continued at home for 24 days. They returned to the clinic to increase the dose and continued this process until reaching up to 4,000mg of sesame protein (about 1 tablespoon worth of tahini). Patients who could tolerate this dose were considered fully desensitized and were instructed to eat 5 grams - a little more than a teaspoon worth - of tahini per day to preserve this desensitization.
After 6 months, 53 of the 60 patients were desensitized to 1 tahini tablespoon worth of sesame protein. During this escalation, there was an adverse reaction in 5% of the induction doses and 2% of the home doses. Epinephrine was used in 10 patients (16%) during the initial hospital-observed phase and in 5 patients (8.3%) for 7 of 253 reactions (2.8%) at home.
The SPT wheal size reduced significantly in the oral immunotherapy group as compared to the control group, but blood IgE levels did not change. The authors concluded that sesame oral immunotherapy “is highly effective, providing full desensitization in 88% and an increase in tolerated dose to greater than or equal to 1200mg in 95% of patients….daily consumption of relatively low daily dose is well tolerated and sufficient to maintain full desensitization.”
Treating anaphylaxis
If desensitization is not done or is not successful, and a reaction turns into anaphylaxis, then epinephrine should be given intramuscularly as soon as possible, and every 5 to 15 minutes until blood pressure improves and symptoms subside. In addition, an antihistamine should be given as soon as possible. In a study of anaphylaxis fatalities, the majority had a severe asthma history and almost all of them did not have an epinephrine injector with them. This was consistent with a retrospective review of 6 fatal and 7 nonfatal episodes of food-induced anaphylaxis in children and adolescents. All subjects who survived had received epinephrine before or within 5 minutes of developing severe respiratory symptoms, and none of the subjects with fatal attacks received epinephrine before the onset of severe respiratory symptoms. This was also consistent with an analysis of data from a national case registry of fatal food anaphylaxis in the United States that indicated only 11% of them had epinephrine autoinjectors available at the time of fatal reaction.
EpiPens are springloaded injectors of epinephrine, which acts as a potent vasoconstrictor that raises blood pressure and bronchodilates, supporting your cardiovascular and respiratory system while the reaction subsides. While they are clearly life-saving devices, they have received much negative press recently for their soaring prices. They are also an awkward size to carry in your pocket and invoke pulp-fiction-needle-stabbing vibes that some people can’t stomach.

These limitations inspired two young twin brothers with severe food allergies, Eric and Evan Edwards, to try to make something better.

In a remarkable success story, after a 15-year journey and a 230 million dollar licensing deal with Sanofi pharmaceuticals, their product hit the markets in 2013 as Auvi-Q, a credit-card-sized auto-injector that talks to you like an automated external defibrillator does, and is preferred of Epi-pens for its simplicity, method of instruction, and device size:
So in summary, sesame seed allergy can range from mild to lethal, but there are highly effective ways to desensitize your allergy. And ALWAYS carry an epinephrine-auto injector. For more on food allergies see FARE.
—
Dr. Larry Istrail is an internal medicine physician and author of The POCUS Manifesto: Expanding the limits of our physical exam with point-of-care ultrasound. You can buy it on Amazon here.