

CT Scans and Radiation Exposure
Are we doing more harm than good?


Dr. Larry Istrail is an internal medicine physician and author of The POCUS Manifesto: Expanding the Limits of our physical exam with point-of-care ultrasound. You can buy it on Amazon here.
—
CT scans are a miracle of modern medicine, enabling us to see our inner organs in high resolution. But these impressive images come at the cost of ionizing radiation exposure. Do they increase our cancer risk?
This is a challenging question filled with emotion and intrigue, the answer to which could have large implications for the future of medical imaging. In order to determine if radiation exposure increases our cancer risk, we take the current estimated cancer risk and add to it the risk associated with each exposure. The lifetime risk of fatal cancer in the general population is about 20% or 400 out of 2,000. The FDA estimates that a 10mSv CT scan will increase your risk of cancer by 1 in 2,000. Adding this extra exposure would increase your cancer risk from 400 chances in 2,000 to 401 in 2,000.
In order to detect such a small increased risk, hundreds of thousands of people need to be studied over a long period of time. Up until recently, no such study had been completed, and our best understanding of ionizing radiation’s toxicity has been gleaned from studying the aftermath of natural experiments.
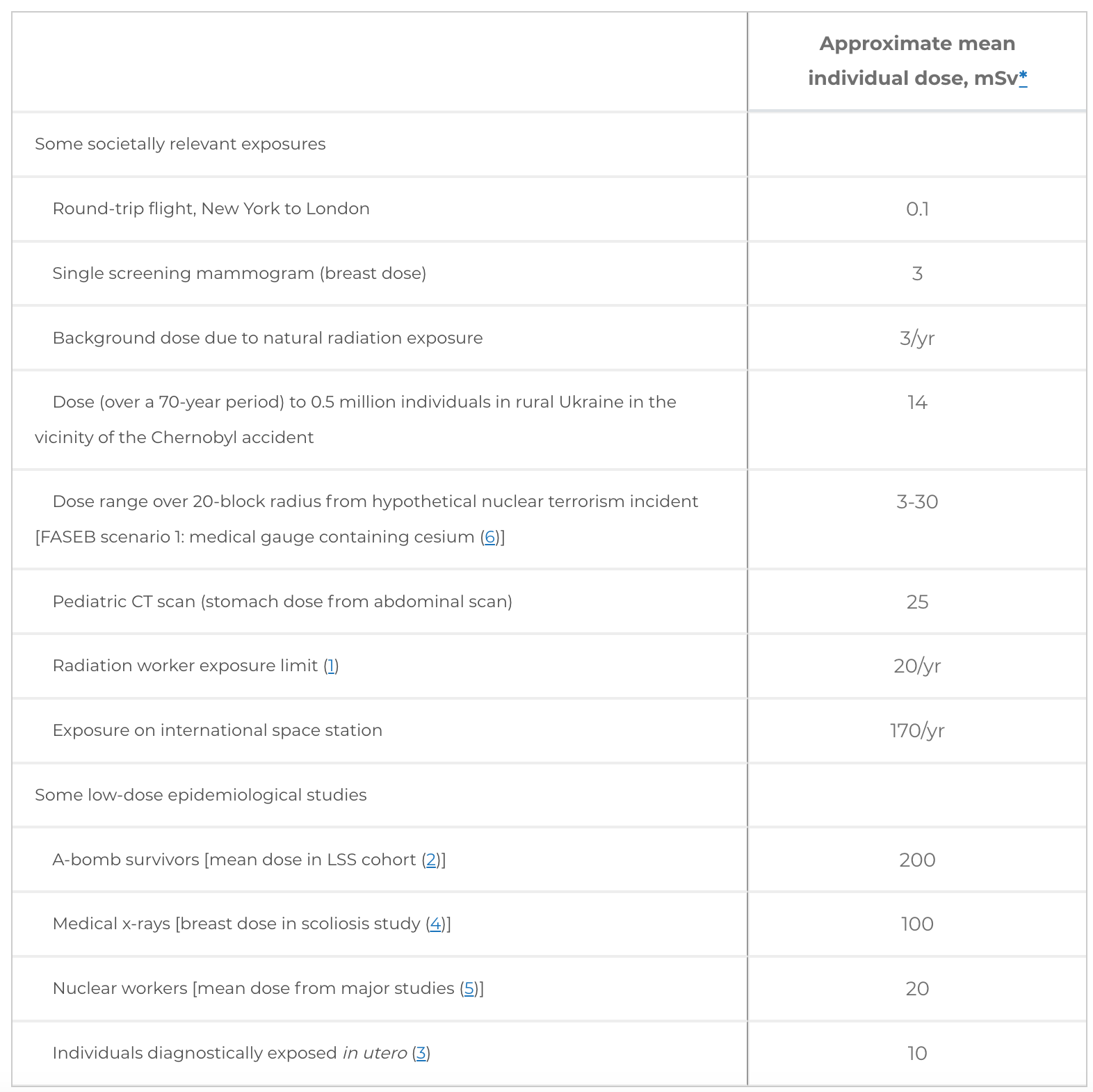
Any excess risk must also be contextualized by the degree of ionizing radiation we are exposed to in every day life. For the average American, it’s about three millisieverts (mSv) of radiation exposure per year, either from radioactive radon gas in our homes or from the cosmic radiation beaming down from the atmosphere. This exposure increases as altitude rises, so a person living in Colorado at 3,300 feet has an annual radiation exposure that is slightly higher than someone living in Washington D.C., at only 410 feet above sea level. Interestingly though, their cancer risk is not higher, and may even be lower through a controversial concept called radiation hormesis, in which a harmful substance in very small quantities may offer beneficial effects to a living organism.
Ionizing radiation risk
Much of what we know about the health risk from ionizing radiation exposure is from following the survivors of historic radioactive atrocities like Hiroshima, or from studies done on nuclear power plant workers. The Hiroshima Bombing on August 6th, 1945 directly killed an estimated 90,000 to 120,000 people, who died instantly from the explosion or from acute radiation poisoning days to weeks later. Although atomic bomb survivors are generally considered an acute large exposure to radiation, the level of exposure varied by how far away a person was at the time of the blast.

The mean dose of radiation of all survivors was only 200 mSv (~6-100 CT scans worth, depending on which scan is chosen for comparison), with more than 50% of the exposed 26,000+ individuals having less than 50 mSv of exposure. When compared to those far away enough to have negligible exposure, individuals exposed to a mean of 34 mSv (ranging from 5 to 125 mSv) showed an increase in solid cancer-related mortality. This was also true in those who lived farther out and had a mean exposure of 29 mSv (range 5 to 100 mSv).
When the data were analyzed from 1958 to 1998 among 105,000 people who were alive, for patients at age 70 after exposure at age 30, solid cancer rates increased by about 35% per Gy of exposure (1 Gy = 1,000 mGy = 1,000mSv) for men and 58% increase per Gy in women. This risk decreased by about 17% per decade from initial exposure.

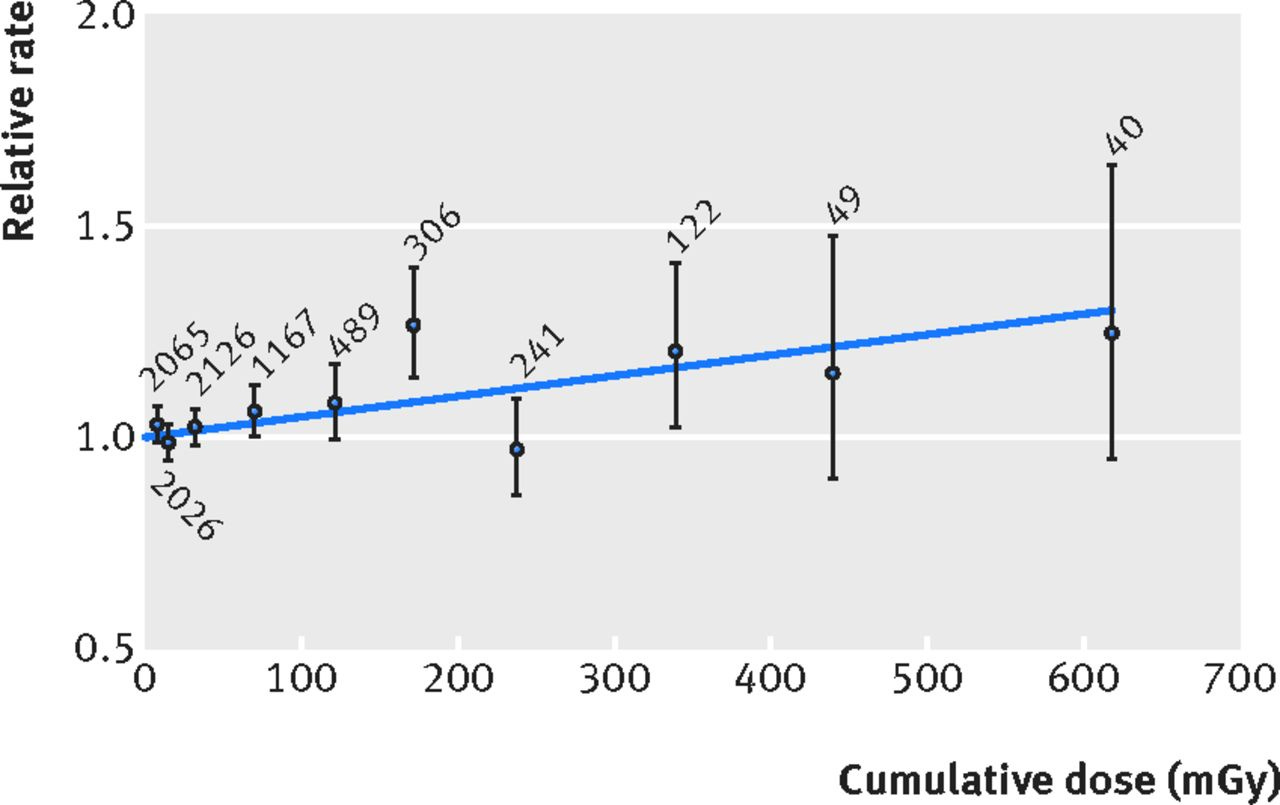
Long term, low dose exposures have also been associated with increased cancer risk. A large study of nuclear energy workers found that they experienced increased rates of blood cancers and solid cancers with just 1.1 mSv of annual and 16 mSv of cumulative excess exposure. This estimated excess relative risk is similar to what was estimated from Hiroshima at comparable radiation doses, with a 47% increased risk for every excess Seivert (1,000 mSv) of exposure. This was notably in a population of 87% men with a median age of 58, so the risks for young people and women would almost certainly be higher.
Medical imaging and cancer risk
In comparison to nuclear power plant workers or atomic bomb survivors, medical imaging exposure is generally - though not always - orders of magnitude lower. A chest x-ray, for example, is only 0.1 mSv, and a mammogram 0.4 mSv, which is about how much an average person would be exposed to naturally over the course of 10 days or 40 days respectively. CT scans emit more ionizing radiation, ranging anywhere from roughly 2 to 31 mSv (or sometimes much higher as we will see) depending on the type and location of the body scanned. This is roughly 20 to 300x more than a chest x-ray, and on par with nuclear energy plant workers or Hiroshima survivors further away from the blast. CT angiogram studies looking for blockages in coronary arteries ranged from 9 mSv to 19 mSv depending on the machine and site in one study, 14 to 15 mSv in another study, or as low as 2.5 mSv from a hospital in Thailand. Despite these relatively high doses of ionizing radiation, with an isolated CT scan the levels of exposure are still generally below the federal occupational recommended annual radiation limit of 50 mSv.
Yet many patients get multiple scans over multiple years and likely accrue far greater exposure than this limit. An emergency department study over 7.7 years and 10,000 emergency room visits found 130 patients that had a CT scan on 3 or more separate emergency room visits. Of those, more than half of them had 10 or more, accumulating more than 91 mSv of cumulative radiation over that period. Using standard extrapolations this would lead to an estimated lifetime risk of developing radiation-induced cancer of one in 110. They highlighted two patients with extremely high cumulative exposures:
A 44-year-old woman with a history of pyelonephritis (kidney infection) and kidney stones with numerous ED visits for flank pain. Over a 20-year period, she had 58 CTs of her ureter, 10 of her abdomen, one of her head, 20 urologic CT imaging scans, 55 abdominal xrays, and 40 chest x-rays resulting in a striking cumulative radiation dose of 1,022 mSv.
A 43-year-old woman with recurrent chest pain had 113 ED visits over 8 years. During that time she had 19 CT scans looking for a pulmonary embolus, 2 chest CTs, 3 abdomen CTs, 2 maxillofacial CTs, 2 head CTs, 1 head and neck CT angiogram, one ventilation-perfusion scan, and 105 chest x-rays resulting in a cumulative radiation dose of 225 mSv.
Such high cumulative doses are especially concerning since they were in young women, who have the highest risk of developing cancer as a result of excess ionizing radiation exposure.
CT scans and radiation doses
CT scans makes up about 11% of procedures that use ionizing radiation but account for 67% of radiation exposure, and the number of CT scans being done is increasing rapidly. Between 1980 and 2007 the approximate number of CTs performed in the U.S. went from 3 million to 70 million. Five to nine million of these scans are performed annually in children, a number that has has increased 8-fold since 1980.
Understanding any potential harm is especially important in younger people, since cancer risks related to radiation exposure decrease as people age. This is both because younger people have more years of life during which a potential cancer can develop, and because growing children are inherently more radiosensitive since they have a larger proportion of dividing cells. Because of these facts, the United States federal dose limit for radiation exposure per year in those under 18 years old is only 5 mSv, 1/10th of that for adults.
Yet according to a study of kids ages 5-14 from 2013, the ionizing radiation exposure from these scans can be far higher, varying from 0.03 mSv to as shockingly high as 69 mSv. A dose of 20 mSv or higher was delivered by 14-25% of abdomen/pelvis scans, 6 to 14% of spine scans, and 3 to 8% of chest scans. They concluded that “many children received high radiation doses from CT associated with a small but significant increase in future cancer risk,” with 1 additional cancer for as few as 300 scans in girls to 660 scans in boys.

These results were similar to a UK study that looked at 74 cases of leukemia and 135 cases of brain tumors in a sample of 170,000+ people. They found that for a scan with typical post-2001 radiation doses in kids under 15 years of age, “cumulative ionizing radiation doses from 2–3 head CTs (ie, ∼60 mGy) could almost triple the risk of brain tumors and … leukemia.” It is important to note that because these cancers are so rare, the overall risk is still very low, even when it is tripled.
For most studies, these cancer risk estimates are based on CT scan manufacturer data which is often calculated on plastic models placed into scanners, or with standardized study protocols that may not be realistic for clinical practice. When radiation exposure is measured in real CT scanners with real people inside them, the doses can be much higher and more variable than expected. A study done at four clinical sites at the University of California San Francisco found that the radiation dose varied widely by the type of CT scan and which portion of the body was imaged. They also found a 6 to 22-fold difference in exposure between repeated scans of the same study. For example, a CT head and neck for suspected stroke exposed patients to a mean of 7.6 mSv at one hospital and a mean of 29 mSv at another. A CT angiogram for suspected pulmonary embolism varied from a mean of 8.1 mSv to a mean of 21 mSv, while for a CT of the abdomen looking for suspected aortic dissection or aneurysm, it ranged from 22 mSv to a disturbingly high mean of 49 mSv (with the range of mSv ranging from 6.4 to 90 mSv!).
“Based on the highest effective dose we observed,” they noted in the discussion, “a 20-year-old female who underwent suspected pulmonary embolism CT, coronary angiography CT, or a multiphase abdomen and pelvis CT could have an associated increased risk of developing cancer of as high as 1 in 80.”

This risk declines substantially with age and in men, but 1 in 80 is disturbing and a far cry from the 1 in 2,000 the FDA cites.
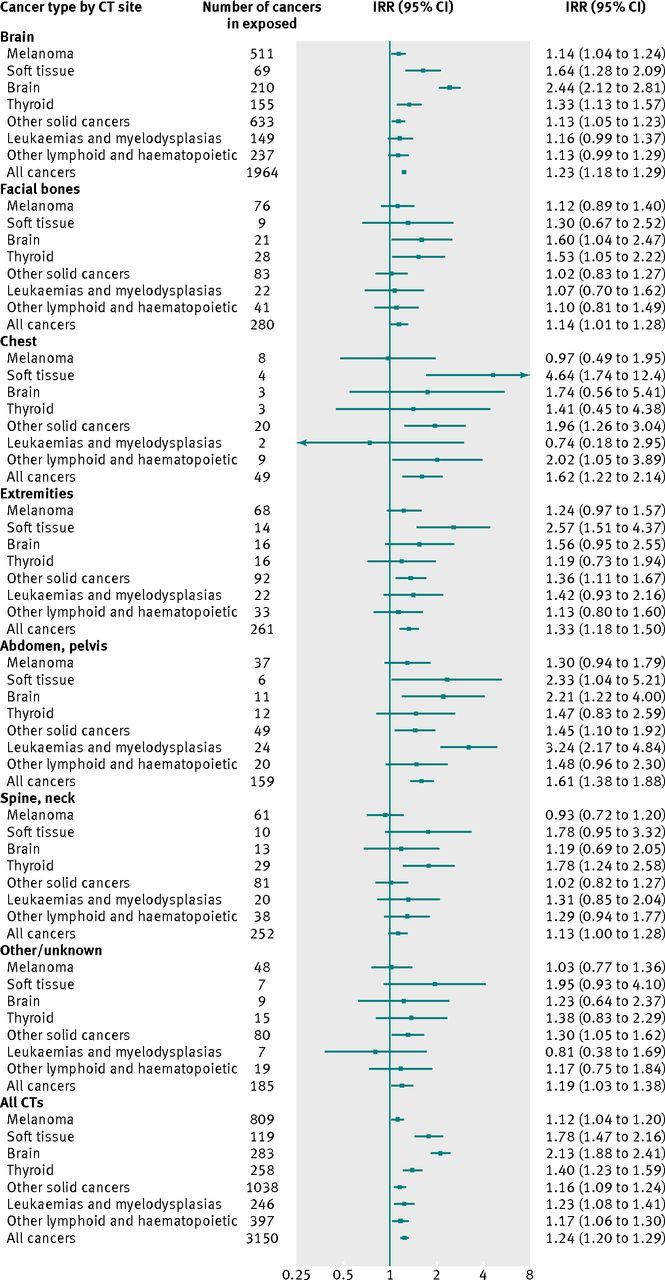
These higher than expected radiation exposures and their potential future harms were further elucidated in the largest study of medical radiation ever done. Published in 2013, it included 680,000 Australians tracked over 20 years and found that “CT scans during childhood and adolescence are followed by an increase in cancer incidence for all cancers combined and for many individual types of cancer.” They looked at people that had one or more CT scans between the ages of 0 and 19. This cohort was compared to over 10 million similar people that did not have any CT scans between 1985 and December 2005. The overall cancer incidence was 24% greater for those exposed, with a dose response of about 16% for each additional CT scan. The risk also increased with reducing age of the patient, with a 35% increased risk for kids ages 1 to 4, down to a 14% increased risk for ages 10-14.
The risks also differed significantly by the site that was scanned and the type of cancer tracked. The largest increases in risk were seen after CT scans of the chest and abdomen (62% and 61% increased risk respectively). CT scans of the brain more than doubled the risk of brain cancer (IRR of 2.44). After scans of the abdomen or pelvis, there was a 3x increased risk for blood and bone marrow cancers. As seen in the figure below, they also noted significantly increased risk for many other cancers including thyroid, solid organ, soft tissue, and skin.
Correlation or causation?
With these large association studies, it is very important to remember the limitations. These cannot definitely prove the radiation from CT scans causes these extra cancers. Patients with unexplained headaches or persistent symptoms due to cancers are more likely to seek out care and get these scans, so there may be some reverse causation here. However, there are multiple factors that support the notion that this ionizing radiation is in fact causing cancer that otherwise would not develop:
There is a known risk of high dose radiation and biological plausibility with lower doses
The relative risk increases with the number of CT scans
The younger the patient when exposed, the higher the risk
Correlation between the site of the CT scan and the cancer
A general agreement among different studies in different decades, countries, and clinical scenarios
These trends were also seen in a large meta-analysis of studies including 111 million people from different countries in which they identified “an inordinately increase in cancer risks from CT scans for adults…the cancer risks were positively correlated with radiation dose and CT sites.”
So, what do we do about it?
From all the evidence to date, it seems that ionizing radiation exposure from CT scans can have a small but real increase in cancer risk, especially in young women. The younger you are and the more scans you have, the higher the risk. The highest observed exposure from the UCSF study corresponds to a risk of 1/80 in a 20-year-old woman. This would increase the risk of developing cancer from the baseline 400 per 2,000 people to 425 per 2,000, which if true, would be very concerning.
Yet this risk must be balanced with the high resolution and high sensitivity and specificity CT scans offer. Sometimes there is no better way to make the correct diagnosis. If a young woman comes to the hospital with tachycardia and chest pain due to a large pulmonary embolus, there are no other direct ways to diagnose a pulmonary embolus. Not ordering a CT angiogram due to possible increased future cancer risk would be the wrong thing to do if she in fact had a life threatening blood clot.
The authors of the UCSF study offer 3 recommendations:
CT examination protocols and techniques should be optimized and standardized to limit the radiation associated with individual scans.
A focus on reducing the number of CT examination (often easier in theory than in practice)
Track and collect dose information at the patient level, as patients may undergo repeated imaging over time
Ultimately, the best solution for reducing CT scans is to train clinicians in using ultrasound. It will not help with organs that ultrasound cannot accurately image (brain, spinal cord) and may only partially help in patients with abdominal pain. But it would dramatically reduce the need for CT scans of the chest. Lung ultrasound in the hands of a skilled clinician can diagnose common lung diseases on par with what a CT scan can do. Every scan has zero mSv of ionizing radiation. Lung ultrasound has already replaced chest x-rays for many years in a NICU in China.
For a young patient that presents with shortness of breath or chest pain, it’s the least we can do.
—
Dr. Larry Istrail is an internal medicine physician and author of The POCUS Manifesto: Expanding the Limits of our physical exam with point-of-care ultrasound. You can buy it on Amazon here.
Thanks for this informative piece! Do you know of any protocols that can help the body handle radiation from scans, either before or after?