
Covid Boosters for Young People: Evidence of Benefit?
Covid Boosters for Young People: Evidence of Benefit?
The vaccines remain remarkably effective for preventing severe disease, so why does everyone need a booster?

Larry Istrail is a physician and author of The POCUS Manifesto: Expanding the Limits of our Physical Exam with Point-of-Care Ultrasound (POCUS). You can buy a copy here.
—
One year into the vaccine rollout, it’s safe to say there’s been remarkable progress yet in some ways it feels bewilderingly the same. Just prior to the vaccine rollout, and prior to knowing how effective the vaccines would be, the general medical consensus was that an effective vaccine rolled out to 70-80% of the population would give us herd immunity and end the pandemic by protecting the vulnerable and reducing transmission.
A study published in October 2020 predicted that “to prevent an epidemic, the vaccine has to have an efficacy … of at least 70% when vaccination covers at least 75% of the population. To extinguish an ongoing epidemic and obviate the need for any other measures (e.g., social distancing), the vaccine has to have an efficacy of at least 80% with a 75% vaccine coverage.”
This was a very reasonable estimate, however, as of December 18th, 2021, in the United States with vaccines that are 85-95% effective and 61% of the population fully vaccinated (73% with at least 1 dose), we have certainly not prevented a reoccurring epidemic. In New York, the epicenter of the U.S. outbreak, with 70% of the population vaccinated and a likely large percentage of the unvaccinated that have natural immunity, they still recorded 20,563 new cases, a record for the entire pandemic. In Ireland, 90% of people over 12 years old are fully vaccinated yet they recorded as many as 5,622 new cases compared to as many as 7,800 about one year prior.
How can this be!?
The concept that mass vaccination can greatly reduce or eliminate transmission, so-called sterilizing immunity, is one that has precedent, yet generally not with most respiratory viruses. With polio or measles, vaccines can reduce spread because these diseases require dissemination throughout the body as necessary for transmission. SARS-CoV2, like other coronaviruses do not. They replicate in the mucosal lining and are transmitted by respiratory droplets, and therefore a vaccination generally cannot prevent such infections.
NIH immunologist Dr. Jonathan Yewdell described herd immunity to COVID-19 as a “pipe dream,” noting that:
What polio-, variola, and measles virus share is dissemination from the initial infection site via lymph and (secondarily) blood as an obligate step in pathogenesis or transmission. Virus-programmed interorgan dissemination occurs in stages over days, as the virus productively infects one organ and proceeds to the next via lymph and blood ... Blood/lymph-based dissemination or tropism is clearly implicated as the critical vulnerability of viruses to infection/vaccination-induced immunity.
While it may not be able to eliminate the virus from the planet, what it can do is protect the lungs and other organs from being involved once it does infect your oral or nasal mucosa. This - as well as the introduction of new variants - is likely why case transmission is not reducing while hospitalization and death are waning dramatically.
For example, using back-of-the-envelope calculations based on confirmed cases and deaths, at Ireland’s peak infection rate of 7,832 cases there were as many as 74 deaths per day, a case fatality rate of about 1%. Since then it has ranged from only 0-12 per day, a 10x reduction to a rate of about 0.1%. In New York, during the January peak of cases, there were as many as 200 deaths per day with a case fatality rate of as high as 1.2% while in November it was roughly 0.4%. Similar reductions in mortality were seen in other extremely highly vaccinated countries like Portugal, Spain, or Italy.
This of course is confounded by many other factors - better management, the introduction of steroids and other treatments, etc. But vaccination status is clearly a main contributor, as confirmed by ICU admission rates of vaccinated patients as compared to unvaccinated:
A Dutch study of 15,000 patients showed 95% risk reduction of hospitalization and 97% risk reduction of ICU admission
A Sept 2021 study of 41,000 adults over 50 years old that found full mRNA vaccination reduced hospitalization by 89%, ICU admission by 90%, and urgent care/emergency department visits by 91%
May 2021 Israeli study of millions of citizens showed over 95% risk reduction for hospitalization, ICU admission, or death across all age groups
May 2021 study from CDC with 94% reduced risk of hospitalization for fully vaccinated adults over 65
August 2021 study found an 87% reduction in risk of hospitalization for fully vaccinated compared to unvaccinated
January - June 2021 study of 4,700 people around the U.S. who required ICU admission for COVID or died in the hospital due to COVID found that despite being significantly older on average (73 years old vs 59), hospitalization rates were 17x higher in unvaccinated patients
An April 2021 study of over 90,000 people in the United States found that among the 225 deaths among Covid-19 hospitalizations, 97% were in the not immunized, 2.2% in the partially immunized, and 1 (0.0041%) in the fully immunized group computing 96% risk reduction in hospitalization and 98% reduction in death
A December 2021 study of 8 million New Yorkers in the New England Journal of Medicine found “effectiveness against hospitalization with Covid-19 among adults 18 to 64 years of age remained almost exclusively greater than 86%, with no apparent time trend, and only declined by about 4-6% in people over 65
A study in North Carolina over 9 months found that full vaccination reduced hospitalizations by 87% and death by 88% at 7 months out
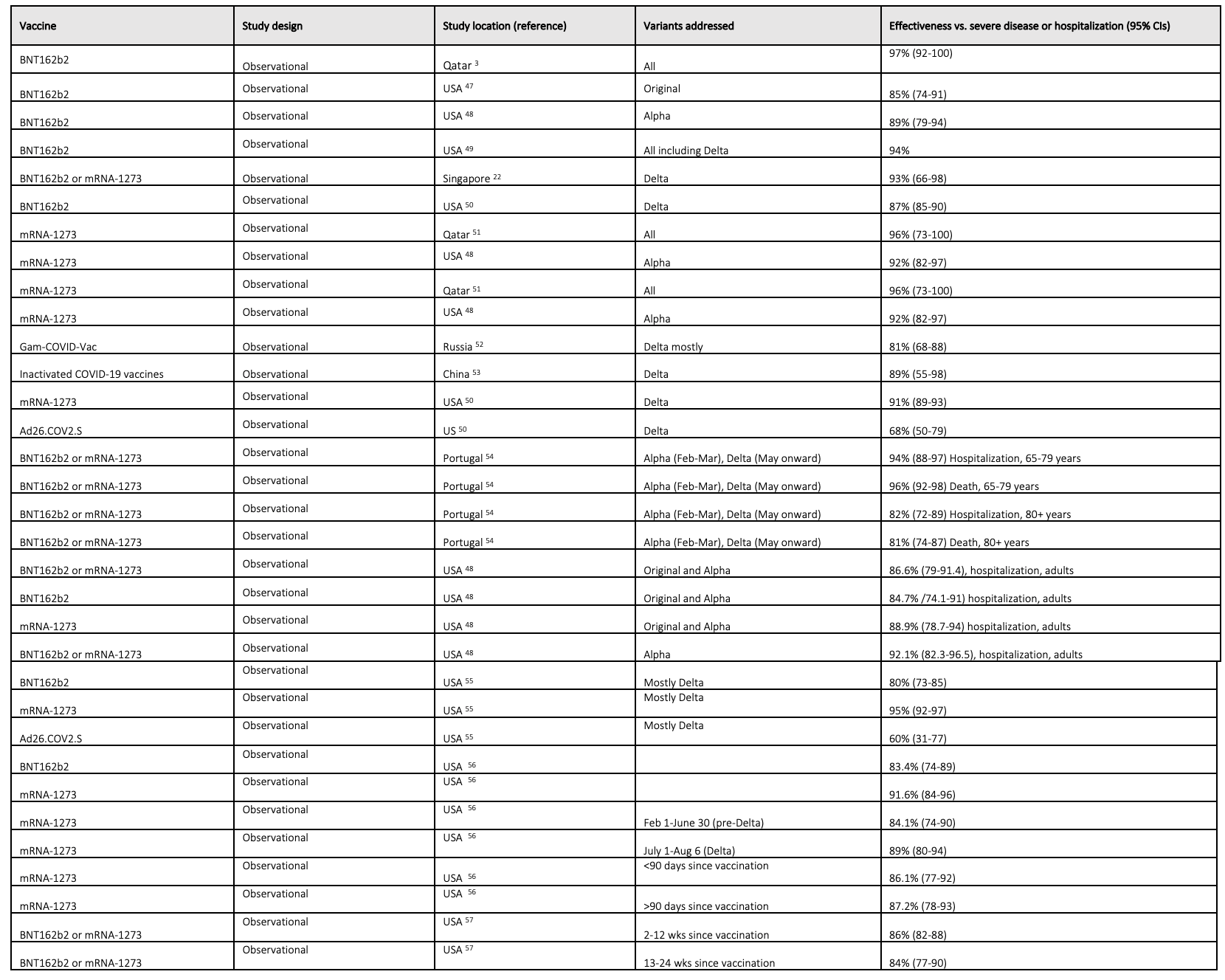
There are many more such studies, summarized in the table below from an Oct 2021 Lancet paper.
Waning Immunity, Breakthrough Infections
To determine if immunity is waning, it is important to clearly define what this means. There is a constant barrage of stories about “breakthrough infections,” yet minimal discussion about what it actually means. AstraZeneca defines it as a case in which a vaccinated person tests positive for SARS-CoV2, as does the CDC which defines it as “when a fully vaccinated person gets infected with COVID-19.”
Yet as we discussed, if it is true that vaccines cannot cause sterilizing immunity to SARS-CoV-2 and don’t prevent transmission anymore (more on this later), then this definition is self-defeating. By this definition, there will always be breakthroughs, especially with new variants and in areas with a high concentration of disease. The vaccine is not a forcefield that hovers around your oropharynx and fruit-ninja’s any viral particles that approach. Rather, it is a seatbelt and airbag for arguably your most precious possession: working lungs.
“We’ve damned the vaccine,” said Paul Offit in an interview, an internationally recognized virology and immunology expert at Children’s Hospital of Philadelphia who sits on the Food and Drug Administration’s vaccine advisory committee. “By using the term ‘breakthrough,’ we’ve implied failure. That even though you’ve been vaccinated, if you get an asymptomatic or mildly symptomatic infection that somehow the vaccine has failed you, when it hasn’t.”
As a more apt analogy, consider car accidents. Over 38,000 people a year die in car accidents in the United States each year, which is a remarkably high number yet in such a big country it is only about 0.01% of the population. Among the many improvements to cars over the years, this low rate is due in large part to seatbelts. They reduce your risk of death in a car accident by about 50% and therefore would be unwise to not wear one. But they don’t prevent car accidents, and judging them by their ability to do so would bring their effectiveness into question.
The same could apply to the COVID vaccines. The goal for these vaccines - or any vaccine - fundamentally is to prevent death or serious illness. In my opinion, everything else is icing on the cake, and judging such a vaccine by its ability to prevent mild infection creates enormous distrust as would judging a seatbelt by its ability to prevent a crash.
Waning immunity studies
As 2021 progressed, evidence was clear that antibody levels were reducing, suggesting that immunity to severe disease may also be waning, especially in those over 65 years old.
But what about in young people? After all, multiple colleges are now requiring a booster shot for their students.
A Dec 9, 2021 study found that in adults over 60, the group who received a booster vaccine had a 1.9/100,000 person-day rate of severe illness (defined as breathing more than 30 times per minute or a resting blood oxygen saturation of less than 94%), while the 2-dose-ers had 5.4/100,000 person-day rate. Notably, they included the following comment in regards to the younger population in the study:
“Only persons 40 years of age or older were included in the analysis of severe disease because severe disease was rare in the younger population.”
This verbiage was also seen in another Israeli study which showed significant benefit for the booster in the older subgroups but in those under 40:
“the rate of severe disease in the youngest age groups is very low and there were not enough cases to compare the rates of severe disease (23 in the non-booster group and one in the 12+ days post booster and in the booster control groups).”
This sentiment was shared by Dr. Paul Offit, the godfather of vaccinology (my designation), in another interview. He has written multiple books on vaccines, co-developed the rotavirus vaccine, and is a member of the FDA vaccine advisory committee. You can hear him discuss boosters for yourself here:
Offit, along with Philip Kraus and Marian Gruber, the former deputy director and director of the FDA's Office of Vaccines Research and Review, wrote a strongly worded Op-Ed opposing boosters for everyone, agreeing that for people over 65, those at high risk, or those who are immunosuppressed they make sense. The latter two also wrote an article in the Lancet summarizing the data, also arguing against boosters for all:
“Current evidence does not, therefore, appear to show a need for boosting in the general population, in which efficacy against severe disease remains high. Even if humoral immunity appears to wane, reductions in neutralising antibody titre do not necessarily predict reductions in vaccine efficacy over time, and reductions in vaccine efficacy against mild disease do not necessarily predict reductions in the (typically higher) efficacy against severe disease.”
On September 24th, the CDC announced the following regarding boosters:
people 65 years and older and residents in long-term care settings should receive a booster shot of Pfizer-BioNTech’s COVID-19 vaccine at least 6 months after their Pfizer-BioNTech primary series,
people aged 50–64 years with underlying medical conditions should receive a booster shot of Pfizer-BioNTech’s COVID-19 vaccine at least 6 months after their Pfizer-BioNTech primary series,
people aged 18–49 years with underlying medical conditions may receive a booster shot of Pfizer-BioNTech’s COVID-19 vaccine at least 6 months after their Pfizer-BioNTech primary series, based on their individual benefits and risks, and
people aged 18-64 years who are at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting may receive a booster shot of Pfizer-BioNTech’s COVID-19 vaccine at least 6 months after their Pfizer-BioNTech primary series, based on their individual benefits and risks.
But shortly after, their website suggests everyone over 18 “should” get a booster. What gives?
Vaccines, viral loads, and transmission
The private sector response to the covid emergency and the resulting vaccines will no doubt go down as one of the most remarkable achievements in scientific history. The persistent protection from severe illness consistent across multiple studies in multiple countries confirms this.
But the other hope for them was that they would also prevent transmission. This, after all, is the reason people feel more comfortable around others who’ve been vaccinated. It is also why there is such concern over unvaccinated people’s ability to spread the disease and prolong the pandemic. As one hospital website described it:
“The good news is that data from the U.S. Centers for Disease Control and Prevention (CDC) shows while COVID-19 infections do occur in fully vaccinated people, these instances appear to be exceptionally rare.
We do not have conclusive proof. But more and more studies and real-world evidence points to fully vaccinated people, who are not immunocompromised, are less likely to transmit the virus if they become infected”
We now know that vaccinated people getting infected is not exceptionally rare at all. Again, based on the principles discussed above, the vaccine is not a forcefield. A vaccinated person in an area of highly concentrated disease can get infected. What’s important is that they are protected from getting extremely ill.
Evidence during alpha variant predominance
Before the Delta variant, multiple studies were done trying to determine if vaccinated people can transmit the virus as well as unvaccinated can. This was generally done by finding vaccinated people who become infected and then testing their household contacts. They then compare this rate to similar unvaccinated, infected people. These studies are very hard to do, are not randomized, and therefore suffer from a lot of potential confounding.
January - February 2021 study in England found that in 960,000 household contacts of infected unvaccinated patients there were 96,000 secondary infections or about 10%. This was compared to 5,900 vaccinated people who were infected that resulted in 371, or 6% secondary infections, concluding that “the likelihood of household transmission was approximately 40 to 50% lower in households of index patients who had been vaccinated 21 days or more before testing positive than in households of unvaccinated index patients.” Though comparing groups that are so different in size is questionable, and they include the important caveat that “studies that involved active follow-up of contacts and that used serologic testing have shown higher rates of household transmission than were observed in our study.”
Another study From December 2020 to April 2021 in Israel tracked the SARS-CoV-2 transmission in the households of 12,518 healthcare workers and they did show a reduction in transmission. Among the 641 household contacts whose index case was unvaccinated, 261 (41%) developed a SARS-CoV-2 infection. This proportion dropped to 19% (8 out of 43) among household contacts whose index case was vaccinated.
Another study suggested there was an 80% risk reduction when exposed to an infected vaccinated person compared to unvaccinated
Yet measuring transmission this way has many potential flaws. The family of an unvaccinated individual may have very different behaviors than those of the unvaccinated. To my knowledge, none of these studies confirm that the infection actually came from the infected family member, as opposed to from an indoor concert they may have attended.
Evidence with the Delta Variant
One hypothesis as to why the vaccine would reduce transmission is that it hinders the replicating ability of the virus and would therefore have lower viral loads that could be passed on to someone else. One of the most thorough studies testing this hypothesis was done on professional basketball players and recently published in the New England Journal of Medicine. They collected 19,941 SARS-CoV-2 viral samples from 173 NBA players between November 28, 2020, and August 11, 2021, and they found “no meaningful difference in the mean peak viral load, proliferation duration, clearance duration, or duration of acute infection of either the alpha or the delta variant … We also found no meaningful difference in the mean peak viral load or proliferation duration between vaccinated and unvaccinated participants.”
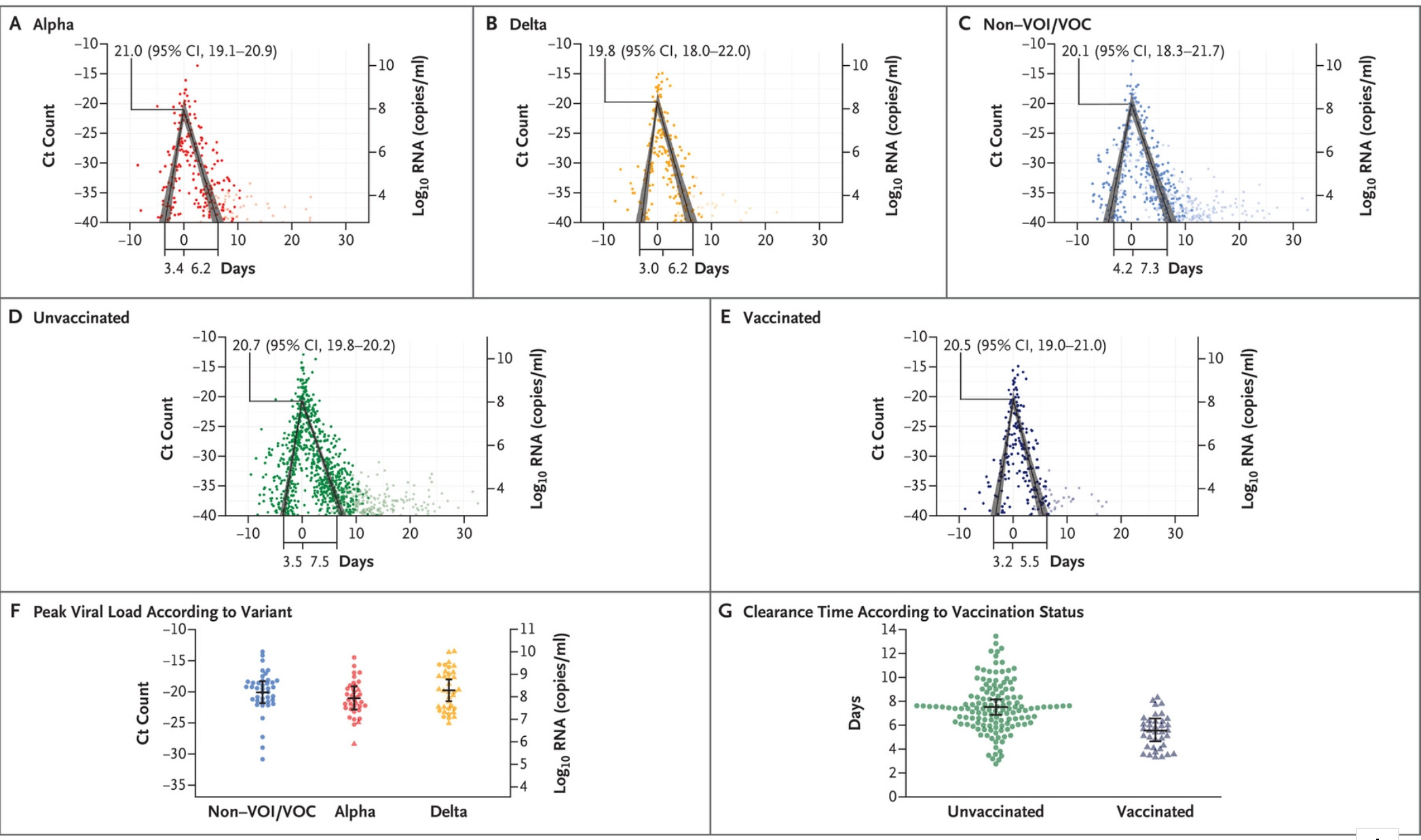
They did, however, find that vaccinated NBA players cleared the virus 2 days faster than the unvaccinated ones. This seems to confirm what was seen in a rigorous study from the UK in September 2021 looking at Delta variant infections.
Close contacts of subjects in this study underwent daily PCR testing with the goal of quantifying “household transmission of the delta variant and assess the effect of vaccination status on contacts’ risk of infection and index cases’ infectiousness.” And their findings do not support the ability of our vaccines to prevent transmission of the Delta variant:
“We identified similar [secondary attack rate] (25%) in household contacts exposed to fully vaccinated index cases as in those exposed to unvaccinated index cases (23%). This finding indicates that breakthrough infections in fully vaccinated people can efficiently transmit infection in the household setting.”
As in the NBA study, they also found no evidence of variation in peak viral load by variant or vaccination status. So if vaccines are highly effective at protecting us from severe disease, but don’t reduce viral load, and don’t seem to prevent transmission anymore, then the idea that boosters are required to prevent transmission confuses me.
Potential myocarditis risk with boosters
The other concern with requiring boosters for college students and young people is what unintended harms it may cause. There are many factors that need to be considered such as overall risk, risk reduction with the booster, and rates of myocarditis from SARS-CoV2 infection in vaccinated young people without a booster. As of June 11, 2021, the CDC reported that:
“Within the Vaccine Adverse Event Reporting System (VAERS), the national vaccine safety passive monitoring system, 1,226 reports of myocarditis after mRNA vaccination were received during December 29, 2020–June 11, 2021. Among persons with reported myocarditis after mRNA vaccination, the median age was 26 years (range = 12–94 years), with median symptom onset interval of 3 days after vaccination (range = 0–179). Among 1,194 reports for which patient age was known, 687 were among persons aged <30 years and 507 were among persons aged ≥30 years; of 1,212 with sex reported, 923 were male, and 289 were female. Among 1,094 patients with number of vaccine doses received reported, 76% occurred after receipt of dose 2 of mRNA vaccine; cases were reported after both Pfizer-BioNTech and Moderna vaccines.”
This is self-reported VAERS data, which sole purpose is to generate hypotheses and possible signals. It is also highly subject to bias and fraud. In the most recent, far more rigorous Danish study on this topic of nearly 5 million people, researchers tracked all patients who received the Pfizer, Moderna, or J&J vaccines. There were 269 people who developed myocarditis, 40% of which were 12-39 years old and 73% were male, and the risk was highest after the 2nd dose of the Moderna vaccine.
They summarized their principal findings:
“We did observe a strong association between vaccination with [moderna vaccine] and myocarditis or myopericarditis, defined as the combined outcome of a hospital diagnosis of myocarditis or pericarditis, increased troponin levels, and a hospital stay lasting more than 24 hours. Vaccination with [Pfizer] was only associated with an overall increased rate of myocarditis or myopericarditis among female participants. In general, the rate of myocarditis or myopericarditis was about threefold to fourfold higher for [Moderna] vaccination than that for BNT162b2 vaccination.”
It’s important to stress that the absolute number of events was still extremely low. In 12-39 year olds, the rate was 1.6 per 100,000 individuals with Pfizer and 5.7 per 100,000 with Moderna. Fortunately, the clinical course of these patients was relatively mild with no readmissions, diagnoses or heart failure, or death.
These results were very similar to a study of over 19 million doses given in Ontario, Canada. Between December 2020 and September 2021, there were 427 reports of myocarditis. Of those, 297 met the official criteria for myocarditis. 77% occurred in males. The highest rates of myocarditis or pericarditis were seen in males aged 18-24 years following 2nd dose of Moderna, which was 5.1 times higher (299.5 per million doses) than the rate following Pfizer as the second dose (59.2 per million doses). The rates were higher in people who had a shorter inter-dose interval of fewer than 30 days compared to those who spaced the doses out by more than 56 days. They concluded that they observed:
“a strong suggestion of a product-specific association; the rates following a second dose of '[Moderna'] were higher than those following a second dose of [Pfizer], in particular for young males. In addition to product-specific insights for age/sex groups at highest risk, our analyses suggest that inter-dose interval and vaccine schedule combinations may also play a role in the risk of myocarditis/pericarditis. These observations suggest that there may be programmatic strategies relating to product, interval, and schedule that could play a role in reducing the risk of myocarditis/pericarditis following mRNA vaccines.”
In Israel in another study with the Pfizer vaccine between Dec 2020 and May 2021, a small but significant myocarditis signal was also seen. During this time period, there were a total of 283 confirmed cases of myocarditis due to any cause. 142 of these occurred within 21 days after the first dose and 30 days after their second. 29 cases were seen in patients with confirmed COVID-19 and 72 without a confirmed diagnosis.
In the 136 people out of the 5 million who received 2 doses of the Pfizer vaccine who had “definite or probable myocarditis,”
“the clinical presentation in 129 was generally mild, with resolution of myocarditis in most cases, as judged by clinical symptoms and inflammatory markers and troponin elevation, electrocardiographic and echocardiographic normalization, and a relatively short length of hospital stay. However, one person with fulminant myocarditis died. The ejection fraction was normal or mildly reduced in most persons and severely reduced in 4 persons. Magnetic resonance imaging that was performed in 48 persons showed findings that were consistent with myocarditis”
The risk was significantly higher in males and highest in people between 16-19 years old with a rate of 13.7 per 100,000 persons, with 90% of the risk attributed to the 2nd dose. They concluded that “in our study, definite or probable cases of myocarditis among persons between the ages of 16 and 19 years within 21 days after the second vaccine dose occurred in approximately 1 of 6637 male recipients and in 1 of 99,853 female recipients.”
Similar results were also seen in a very large study out of the United Kingdom between Dec 2020 to August 2021. They looked at all hospital admissions for myocarditis and looked for associations between SARS-CoV2 infection and vaccination.
During this period there were about 1600 myocarditis and 1500 pericarditis-related admissions or deaths.
Myocarditis
Of the 38 million vaccinated people, 397 admissions or death related to myocarditis were recorded 1-28 days post any dose. This was much more likely after the second dose of the Moderna vaccine, especially in those under 40 years old. In fact, in that age group, the risk of myocarditis from 2nd dose of Moderna was higher than that from a Covid infection. The risks after Pfizer were much smaller.
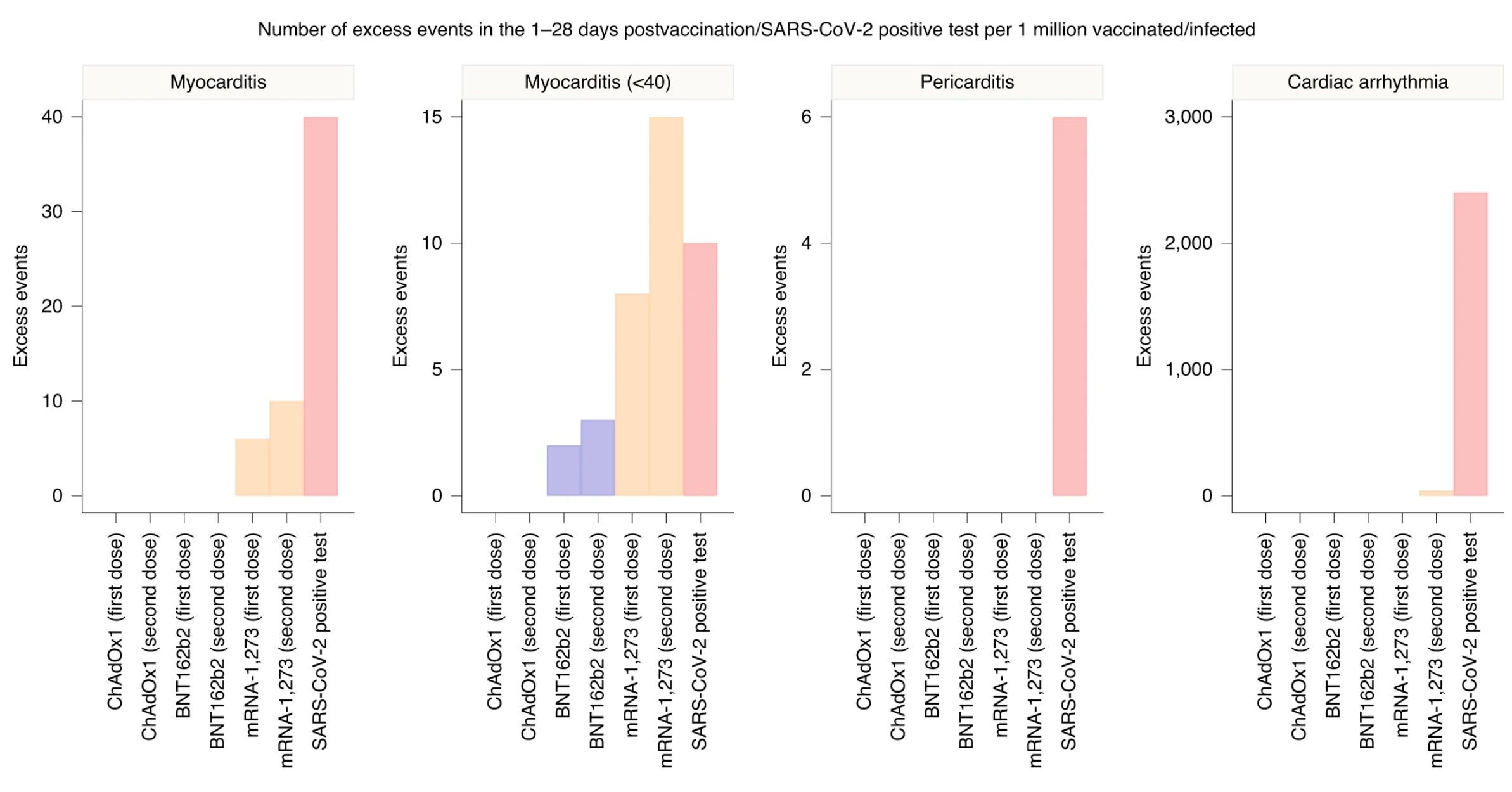
They summarized the results as follows:
For those under 40 years old, the highest risk of myocarditis was 1-28 days following the second dose of Moderna. This resulted in an absolute risk of 15 excess cases per million after the second dose of Moderna compared to 10 cases after COVID infection
In those over 40, the risk of myocarditis was significantly higher from getting COVID than from any vaccine
In men, the highest myocarditis risk was from 2nd dose of Moderna, a smaller but still significant increased risk after covid infection, and no association with Pfizer
In women, the highest risk of myocarditis was after covid infection, with negligible inc risk from vaccines
I am by no means an expert in virology or immunology. I am just a physician who is curious about what the data say about the persistent effectiveness of covid vaccines, and the benefits or possible risks of recommending a booster for young people. What remains clear is that the vaccines are tremendously effective at doing their most fundamental job: preventing severe illness or death, and their benefits should be marketed as such. This is especially true in people under 65 where there does not appear to be any evidence of waning immunity against severe disease. With the small but significant risk of myocarditis in young males, especially after the second dose of the Moderna vaccine, requiring boosters to reduce their already minuscule risk after 2 vaccinations while likely not preventing transmission is a university policy that may need more consideration.
As with everything with COVID, every day is a new surprise, and what is true now may be wrong in 2 months. Let’s hope this all ends soon.
—
Larry Istrail is a physician and author of The POCUS Manifesto: Expanding the Limits of our Physical Exam with Point-of-Care Ultrasound (POCUS). You can buy a copy here.